According to the Centers for Disease Control and Prevention (CDC), 46 people in the U.S. die from an overdose of prescription painkillers every day.[1] Deaths from prescription painkiller overdoses have increased more than 400% among women and 265% among men since 1999.[2] These kinds of statistics have been published across media channels over the past year and have prompted legislative action or dialogue across the U.S.
Now the CDC has published a new study indicating kinship between overuse of drugs such as opioids and marijuana to an alarming increase in heroin use, particularly among demographic groups not linked to heroin use in the past. According to the study, posted in a CDC Vital Signs release on July 10, 2015, heroin use in the U.S. increased 63% from 2002 through 2013. One remarkable finding of the study is that heroin use, historically considered a fringe society drug, has increased among a broad range of demographics, including men and women, most age groups and all income levels – as is the case with opioid drug abuse.
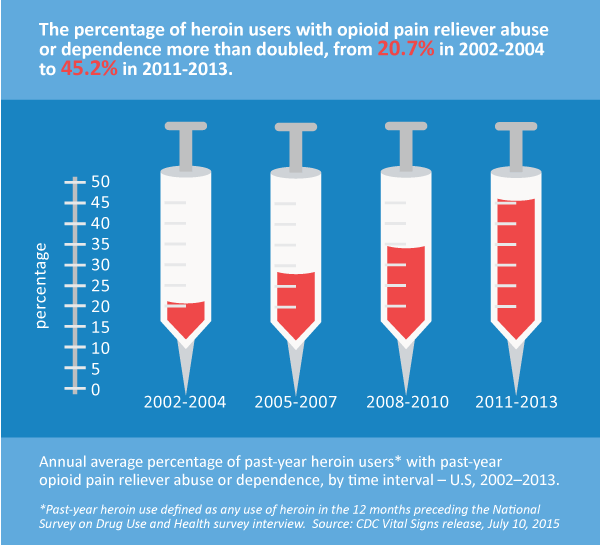
The report indicates that abusers of opioid pain killers are 40 times more likely to be heroin abusers, compared to cocaine abusers who were 15 times more likely to be heroin abusers. Also, 59% of the heroin-related overdose deaths in the U.S. involved at least one other drug. One of the primary conclusions of the study is that there is a very strong correlation between use and abuse of heroin and opioid pain relievers.
Dr. Teresa Bartlett, Senior Vice President, Medical Quality at Sedgwick, said that clinical programs must consistently identify cases in which drugs are not being taken as prescribed. Injured employees receiving opioid medications must be consistently monitored for compliance. Diversion of medications creates dangerous situations in which opioid pain relievers are provided to family members or individuals in the community for non-medical use.
Risk managers and safety managers should consider these trends and make sure their claims administrators are implementing the safeguards necessary to close this potential gateway by preventing prescription drug abuse. Prevention measures include:
- Prescription drug point-of-sale intervention by a trained clinician, pharmacist or peer physician when a prescription drug does not correlate with the injury diagnosis or if it is a chronic pain stage drug being prescribed for an acute injury. Referrals and diagnosis-based formularies with the pharmacy benefit management network are necessary for consistent intervention.
- Peer intervention for prescriber education and alternative treatment negotiation for claims in which drugs have been provided for long-term chronic pain.
- Identification of cases where potential diversions are occurring through systematic and strategic deployment of drug compliance testing to ensure that injured employees are taking medications as prescribed. We strongly recommend you have a written best practices policy for urine drug screening.
- Assistance for long-term chronic users of opioid pain relievers through transfer of care or referral to abuse treatment when necessary.
- Involvement of a behavioral health specialist, who can engage with injured workers being weaned from long-term opioid use for chronic pain. The specialist can identify risk factors for turning to illicit drugs in addition to providing behavioral management tactics.
- Use of a Prescription Drug Monitoring Program by healthcare providers to evaluate their patients’ prescription drug use.
- Use of an Opioid Agreement with injured employees and their prescribers as a standard part of claims management and case management.
According to Eddy Canavan, VP, Workers’ Compensation Practice and Compliance for Sedgwick, it is unlikely that a heroin addiction could become a compensable extension of a workers’ compensation injury. However, this is an untested area and employers should review their claims administrator’s and pharmacy benefit management networks’ clinical drug intervention programs to mitigate risk and to protect the health and safety of their injured employees.
Some opioids and heroin share another common risk: exposure to HIV infection. An HIV outbreak was recently documented in rural Indiana and linked to injectable Opana, an opioid made more potent when crushed, dissolved in water and injected. According to a New York Times update, nearly 150 cases of HIV were documented in rural Indiana as a result of users sharing needles to inject Opana.[3] Insurers and employers must be vigilant to know where the drugs they are buying for injured workers are going.
Safety and risk leaders should act now to make sure drug prevention and health safety practices in claims and case management are aligned to safeguard their injured employees from this alarming trend.
James Harvey, SVP, Managed Care Products & Product Development