A portrait of opioid use disorder

Read part one of Rachel's story here.
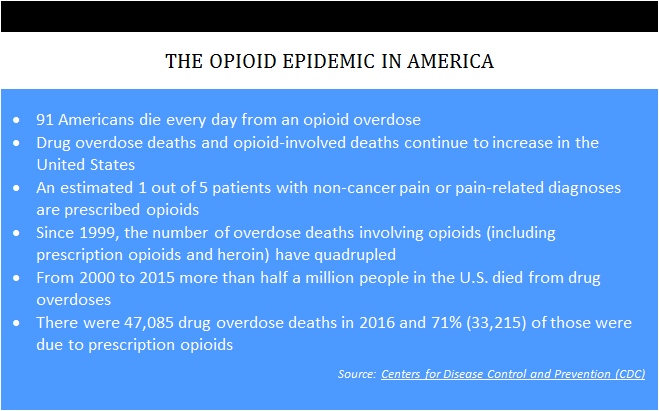
Rachel was once a vibrant gardener, grandmother and worker. Regrettably, following an injury, she became one of a growing number of those suffering from opioid use disorder (OUD). According to the Centers for Disease Control and Prevention (CDC), OUD has grown faster among women than among men in recent years. CDC VitalSigns reported earlier this year that every three minutes, a woman goes to the emergency department for prescription pain-killer misuse or abuse.
However, Rachel’s employer worked with a new claims administrator to implement a drug intervention program that utilized a data analytics tool designed to identify claims with adverse prescription drug trends. This tool quickly identified Rachel as at risk. Her case was flagged because of conditions including multiple prescribers, long-term opioid use, polypharmacy (the simultaneous use of multiple drugs for one patient) and a complicated drug regimen.
John, the new adjuster assigned to the case, agreed that a referral was badly needed. Reema Hammoud, PharmD, was assigned to review the case and put together a weaning plan. Rachel resisted because the pain she experienced was real and the withdrawal symptoms she had experienced when she previously tried to stop taking the opioids were intolerable. Dr. Hammoud identified two conditions of Rachel’s case: 1) analgesia, an opioid induced sense of pain that escalates pain sense and increasing dosage requirements over time, and 2) dependence, a state in which an individual only functions normally in the presence of the drug. When the drug is withdrawn, several physiologic reactions occur. This is known as the withdrawal syndrome. In the case of an opioid, withdrawal can be very serious and the abuser will use the drug again to avoid the withdrawal symptoms.
Rachel’s primary care physician read Dr. Hammoud’s assessment and weaning recommendations and agreed. Rachel’s resistance was extremely strong in the beginning, so John and Dr. Hammoud collaborated frequently.Dr. Hammoud advised Rachel of what to expect and recommended ways to deal with the withdrawal symptoms. Opioids dosages were slowly tapered to minimize withdrawals, and Aubrey, a nurse case manager, was assigned to provide pain coaching.
At the beginning of the weaning period, Rachel made dozens of threatening phone calls to John, Dr. Hammoud and Aubrey. However, over time and with team support, Rachel found that her motivation for self-improvement gradually grew, and John, Aubrey and Dr. Hammoud began to see Rachel emerge from her dependency. At the end of the weaning period, Rachel called each member of the team to say thank you for helping her get her life back.
Today, Rachel once again takes walks with her grandchildren, her garden is thriving, she has a new sense of awareness, and she is very grateful for her changed life.
As this example shows, employers can be societal leaders in the effort to eliminate the opioid epidemic, which is now officially a national emergency. Following a few simple steps can save and restore lives and close cases like Rachel’s:
- Enact automated indicators to identify adverse drug trends.
- Enable PharmD’s to provide expertise in developing weaning plans.
- Connect the adjuster, any assigned nurse, and the PharmD to provide collaborative support.
Authorize only safe and appropriate prescription drugs via routine pharmacy utilization review.
Dr. Reema Hammoud, PharmD, BCPS, Director, Clinical Pharmacy