In recent years, some innovative healthcare leaders and organizations have developed and implemented formal communication and resolution programs (CRPs) that, when combined with advances in patient safety, exemplify fairness and build trust. The intent of CRPs is to lower malpractice costs and maintain patient trust in the healthcare system.
One program in particular, implemented by the University of Michigan Health System, is multifaceted and involves not only open communication about adverse events but also the following (1):
- A critical investigation of the event to determine if the care provided met the standard of care and was reasonable under the circumstances
- An apology to the patient
- Early offer of compensation or settlement, when the care fell below standard or was deemed not to have been reasonable.
Known as “The Michigan Model,” the UMHS program has reported success in reducing malpractice claim costs. An important aspect of this model is the critical investigation by the risk management department at UMHS that leads to a multidisciplinary committee review of the event (or claim) to determine whether the care provided was medically reasonable and if the care had an adverse effect on the patient’s outcome. The event may or may not be referred to peer review, but it is always evaluated for learning opportunities and quality improvement so as to prevent a similar event from occurring again. ASHRM has described a model with similarities in regard to classification and culpability decision making about preventable harm events. [See: ASHRM. Serious Safety Events: A Focus on Harm Classification: Deviation in Care as Link. Getting to Zero™ White Paper Series — Edition No. 2: ashrm.org/pubs/files/white_papers/SSE-2_getting_to_zero-9-30-14.pdf]. It is important to note that the outcome of the investigation is communicated to the patient. When the care was deemed to meet the standard of care and to have been reasonably provided, no compensation is offered and, if a claim is brought, the care is rigorously defended.
Other factors favorable to the success of the UMHS program is that under Michigan law there is a six-month waiting period before the patient can file a lawsuit. This provides time for the investigation and committee review to take place. Also, the committee’s review of the event is protected from legal discovery in that state. After several years of refinement, UMHS reported a claims rate more than 25 percent lower after implementation of its program and a decrease in average monthly cost rates for total liability, patient compensation and non-compensation related legal costs (2).
However, limitations cited for the Michigan Model’s results include that the state of Michigan enacted malpractice reform with caps on noneconomic damages, a six-month mandatory pre-suit notice period and certain expert witness requirements that resulted in an overall reduction in malpractice claims statewide during the UMHS study period.(3) In addition, UMHS is a well- resourced, closed health system that employs its physicians and owns its own captive insurance company—giving it a degree of control over its providers and liability program operations that many healthcare organizations do not have.
CRPs: Successes and Challenges
Two different types of CRPs have evolved. One, an early settlement model, such as the Michigan Model, and another, a limited reimbursement model, which is much more limited in scope with payouts not exceeding a modest amount such as $30,000 to cover out-of-pocket expenses, daily loss of time and sometimes write-off of medical bills. With the limited reimbursement model, patients do not waive their right to sue, as they do with early settlement. (4)
While most, if not all healthcare organizations have implemented disclosure communication following medical error, there are few published reports about organizations that have implemented either type of resolution program or the effects of the programs on malpractice costs. An exception is a Colorado malpractice insurance company COPIC and its limited reimbursement program called the 3Rs program — Recognize unanticipated events; Respond soon after the event occurs and Resolve any related issues. After its first five years in existence, COPIC’s 3Rs program reportedly had a 50 percent drop in malpractice claims against its insured physicians and a 23 percent reduction in claim settlement costs. (5)
One reason for the dearth of published reports of cost savings with CRPs programs may be that CRPs take several years to fully implement and even more time to determine the program’s effectiveness in reducing malpractice claims costs. Even the UMHS program took seven to 10 years to demonstrate cost savings or a reduced rate of cost increases over time. However, programmatic results from early CRPs adopters offer some insights into success factors as well as barriers to implementing an effective CRP. Researchers that studied CRPs reported the following factors contributing to their success (6)
- Executive leadership support and a key champion who is passionate about making the CRP work
- Dedicated human, educational and system resources
- CRP design based on the organization’s structure, culture and needs
- Knowledge about regulatory compliance such as reporting requirements for the National Practitioner Data Bank and state medical/licensing boards
- Readiness for gradual but transformational culture change that takes place over time in order to reap returns on investment in a CRP.
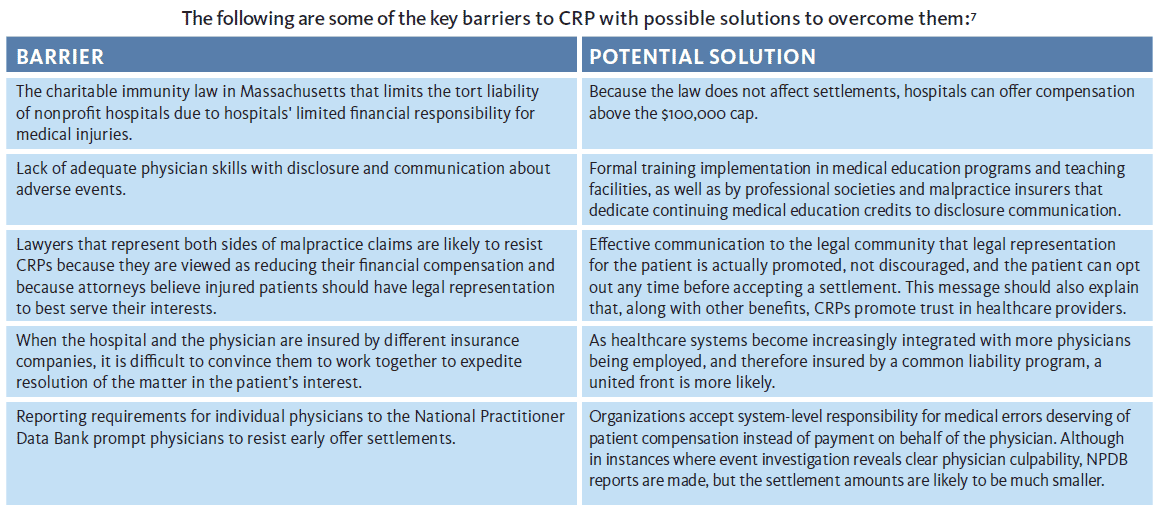
Other investigators of disclosure, apology and offer programs reporting on barriers and strategies for broad implementation offered several insights on CRPs. Although focused on Massachusetts, findings may apply in other states. The following are some of the key barriers to CRPs with possible solutions to overcome them. (7)
Summary
Seventeen years after the IOM report on medical errors and institution of accreditation standards requiring communication of unanticipated outcomes to patients, the logical next step of compensating injured patients fairly and without undue delay when medical care falls below standard or was not reasonable under the circumstances has not been widely achieved. To date, there is limited evidence for the return on investment in CRPs, even with the positive results shared by UMHS about its early settlement model and by COPIC about its limited reimbursement model.
In today’s rapidly evolving healthcare environment, the need to demonstrate value in terms of safety and quality has never been more apparent. As payment for healthcare services based on performance increases, better outcomes become the expectation for patients and health insurers. Informed and engaged patients demand transparency as well as restitution when medical errors result in harm. As barriers are overcome, adding offers of fair compensation to disclosure and apology through formal CRPs, when care is deemed not reasonable or substandard, could ultimately become the norm. In 2017, the Agency for Research and Quality published the CANDOR toolkit (Communication and Optimal Resolution) to assist healthcare organizations in implementing CRPs (ahrq.gov/professionals/quality-patient-safety/patient-safety-resources/resources/candor/introduction.html). Risk managers are poised to take a leadership role in achieving safe and trusted healthcare and CRPs offer a structure and approach to work to that end.
Originally published in the ASHRM Forum newsletter, June 28, 2017: https://forum.ashrm.org/2017/06/28/communication-and-resolution-programs-where-are-we-now/
- The Michigan Model: Medical Malpractice and Patient Safety at UMHS. Retrieved from: http://www.uofmhealth.org/mich...
- Kachalia A., et al., (2010, August 17). Liability claims and Costs Before and After Implementation of a Medical Error Disclosure Program. Annals of Internal Medicine; 17; 153(4):213-21.
- Ibid.
- Mello, MM., et. al. (2014, January). Communication and Resolution Programs: The Challenges and Lessons Learned from Six Early Adopters. Health Affairs; 33(1):20-29.
- Boothman, RC, et. al., (2009, January).A Better Approach to Medical Malpractice Claims? The University of Michigan Experience. J Health Life Sci Law; 2(2):125-159.
- Ibid.
- Bell, SK, et. al. (2012). Disclosure, Apology, and Offer Programs: Stakeholders’ Views of Barriers to and Strategies for Broad Implementation. The Milbank Quarterly; 90(4):682-705.
Kathleen Shostek, RN ARM FASHRM CPHRM CPPS, is vice president, Healthcare Risk Management, Sedgwick